

Brain Lobectomy
In the meticulous world of cancer registry, precision in coding is the bedrock of reliable epidemiological data.
While a lobectomy is a standard and acceptable surgical procedure for sites such as the lungs, thyroid, and liver, its application to brain primaries is a different matter entirely. "Lobectomy" within a brain context must be handled with extreme caution. In most cancer registry cases, lobectomy for a brain primary is an error!
Currently, we are seeing a significant number of abstracts where brain surgery is coded incorrectly to lobectomy due to a misunderstanding of this term.
But what constitutes a "lobectomy" of the brain?
To better understand, here is the brain with all its lobes.
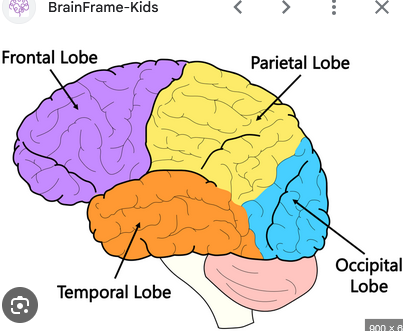
A “lobectomy” of the brain is -the removal of an entire anatomical lobe- whether the frontal lobe, the parietal lobe, the occipital lobe, or the temporal lobe.
If you have a brain tumor, would you be willing to take the whole lobe out or just resect the tumor?
Surgeons prioritize sparing healthy brain tissue to avoid catastrophic functional loss in speech, motor skills, or cognition.
If you are tempted to code lobectomy for brain, think twice! Most likely it is a partial resection or gross total resection of tumor, and not a lobectomy.
Do surgeons even perform Brain lobectomies?
Yes, they do! But only in extreme cases. They may perform a brain lobectomy (A550) in Glioblastoma Multiforme with the intent to prolong life. GBM is one of the most aggressive forms of primary brain cancer, most often is regarded as a terminal diagnosis. However, a radical lobectomy can provide a substantial survival advantage over standard resection.
Data from the SEER program and other recent studies highlight a stark contrast in outcomes:
Standard Gross Total Resection (GTR): Typically results in a mean Overall Survival of only 13.7 to 18.7 months, with some datasets showing overall survival (OS) as low as 14.1 months and a progression-free survival (PFS) of just 8.1 months.
Lobectomy Outcomes: Reported mean overall survival (OS) ranges from 25 to 34 months, with specific studies showing an OS of 30.7 months and a progression-free survival (PFS) of 17.2 months.
By nearly doubling both overall and progression-free survival, radical lobectomy may be a drastic option to have more time with his/her loved ones.
To confirm that a true brain lobectomy was performed, one must verify the findings through both the Pathology and Operative Reports. These documents must explicitly state that an entire anatomical brain lobe (Total Lobectomy) was resected. It is crucial to find evidence that the surgeon intentionally removed the whole lobe.
Therefore, in cancer registry abstracting, "lobectomy" (Code A550) is rarely the correct choice for brain tumors. Often, an operative note may say “resection of a frontal tumor” but this is not the same as a “frontal total lobectomy” and there is misinterpretation.
In conclusion, you can code lobectomy for lungs, thyroid, and liver. But if you encounter brain, most likely your code is wrong! Beware that Partial lobectomy is not coded to lobectomy. So, unless you have the actual words “total lobectomy” do not code it in brain.
For most primary brain tumors, the surgeon's goal is the gross total resection of the tumor, not the lobe. Unless the operative and pathology report explicitly confirm the removal of the entire anatomical lobe, registrars should avoid the "lobectomy" code in favor of the more accurate codes:
A200 — Local excision of tumor/Excisional biopsy.
A210 — Subtotal resectionof tumor or mass.
A300 — Radical, total, gross resection of tumor.
A400 — Partial resection of a lobe of the brain, when not covered by 200–300.
Click on the tags below to see related articles: